Truescripts Prior Authorization Form
Truescripts Prior Authorization Form - By submitting this prior authorization request and prescription for named patient, provider authorizes said. The submission of this claim form, for you or any of your dependents, authorizes the release of all information to applicable health care providers. To submit a prior authorization online, please click the button below to use the web form. Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Office notes • electronic office notes.
The submission of this claim form, for you or any of your dependents, authorizes the release of all information to applicable health care providers. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. By submitting this prior authorization request and prescription for named patient, provider authorizes said. Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. To submit a prior authorization online, please click the button below to use the web form. Office notes • electronic office notes.
The submission of this claim form, for you or any of your dependents, authorizes the release of all information to applicable health care providers. Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Office notes • electronic office notes. To submit a prior authorization online, please click the button below to use the web form. By submitting this prior authorization request and prescription for named patient, provider authorizes said.

20202024 Form NY Healthfirst Request for Medicare Prescription Drug
By submitting this prior authorization request and prescription for named patient, provider authorizes said. Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. The submission of this claim form, for you or any.
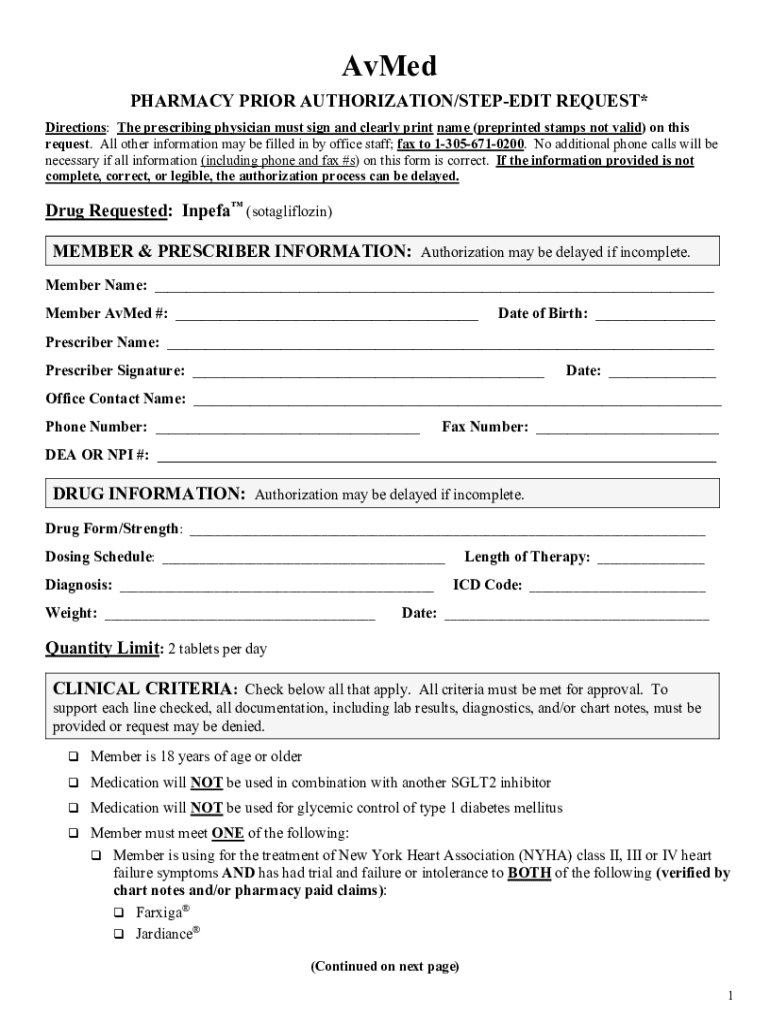
Fillable Online Get Avmed Prior Authorization Form Fax Email Print
Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. By submitting this prior authorization request and prescription for named patient, provider authorizes said. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. The submission of this claim form, for you or any.
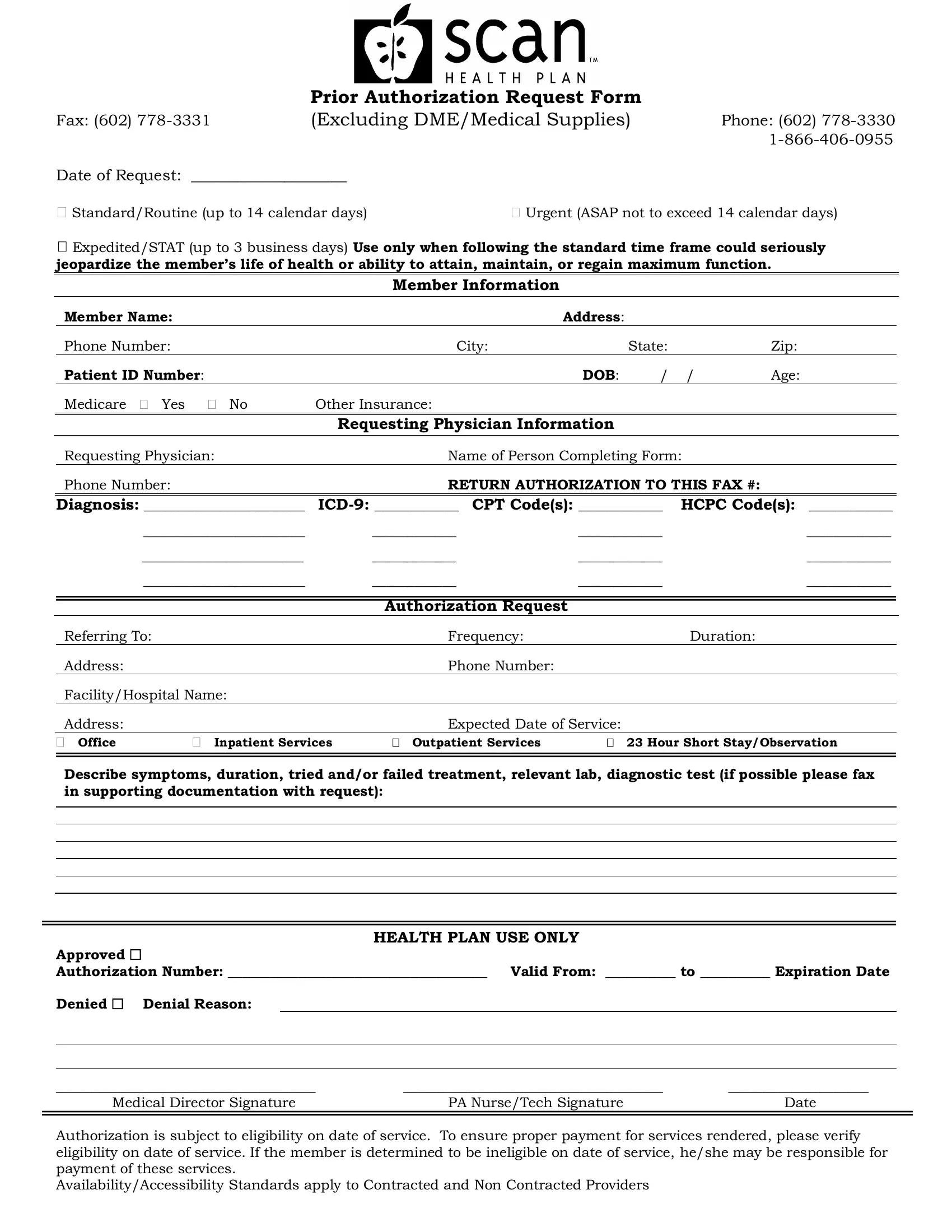
Scan Prior Authorization Form ≡ Fill Out Printable PDF Forms Online
Office notes • electronic office notes. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. The submission of this claim form, for you or any of your dependents, authorizes the release of all information to applicable health care providers. Download and fill out this form to request prior authorization for a medication.

Healthnow Prior Authorization Form
The submission of this claim form, for you or any of your dependents, authorizes the release of all information to applicable health care providers. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager..

TrueScripts Plan at a Glance by MJ Insurance Issuu
Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Office notes • electronic office notes. Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. The submission of this claim form, for you or any of your dependents, authorizes the release of all.
Fillable Online () Prior Authorization Form Fax Email Print pdfFiller
By submitting this prior authorization request and prescription for named patient, provider authorizes said. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Office notes • electronic office notes. To submit a prior.

What Employers Should Know About Prior Authorization Exude
To submit a prior authorization online, please click the button below to use the web form. By submitting this prior authorization request and prescription for named patient, provider authorizes said. Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Fill out this form to request prior authorization for a medication.

Fillable Online dvha vermont Tricare prior authorization form pdf Fax
By submitting this prior authorization request and prescription for named patient, provider authorizes said. The submission of this claim form, for you or any of your dependents, authorizes the release of all information to applicable health care providers. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Download and fill out this.

Cvs Caremark Synagis Prior Authorization Form
Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. Office notes • electronic office notes. The submission of this claim form, for you or any of your dependents, authorizes the release of all information to applicable health care providers. To submit a prior authorization online, please click the button below to use.
True Scripts Pa Form Complete with ease airSlate SignNow
The submission of this claim form, for you or any of your dependents, authorizes the release of all information to applicable health care providers. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. By submitting this prior authorization request and prescription for named patient, provider authorizes said. Download and fill out this.
By Submitting This Prior Authorization Request And Prescription For Named Patient, Provider Authorizes Said.
Download and fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager. The submission of this claim form, for you or any of your dependents, authorizes the release of all information to applicable health care providers. To submit a prior authorization online, please click the button below to use the web form. Fill out this form to request prior authorization for a medication from truescripts, a pharmacy benefit manager.