Printable Medical History Form For Dental Office
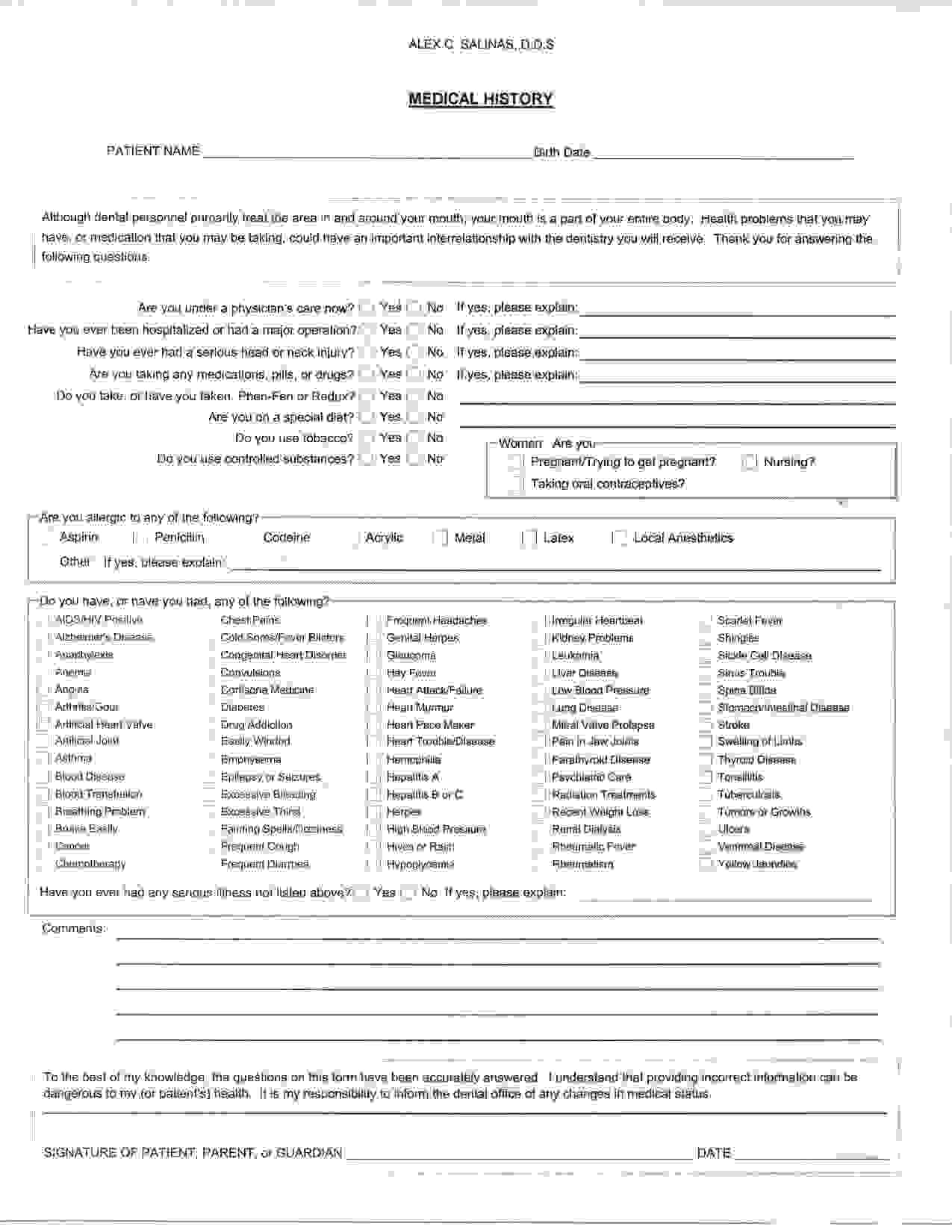
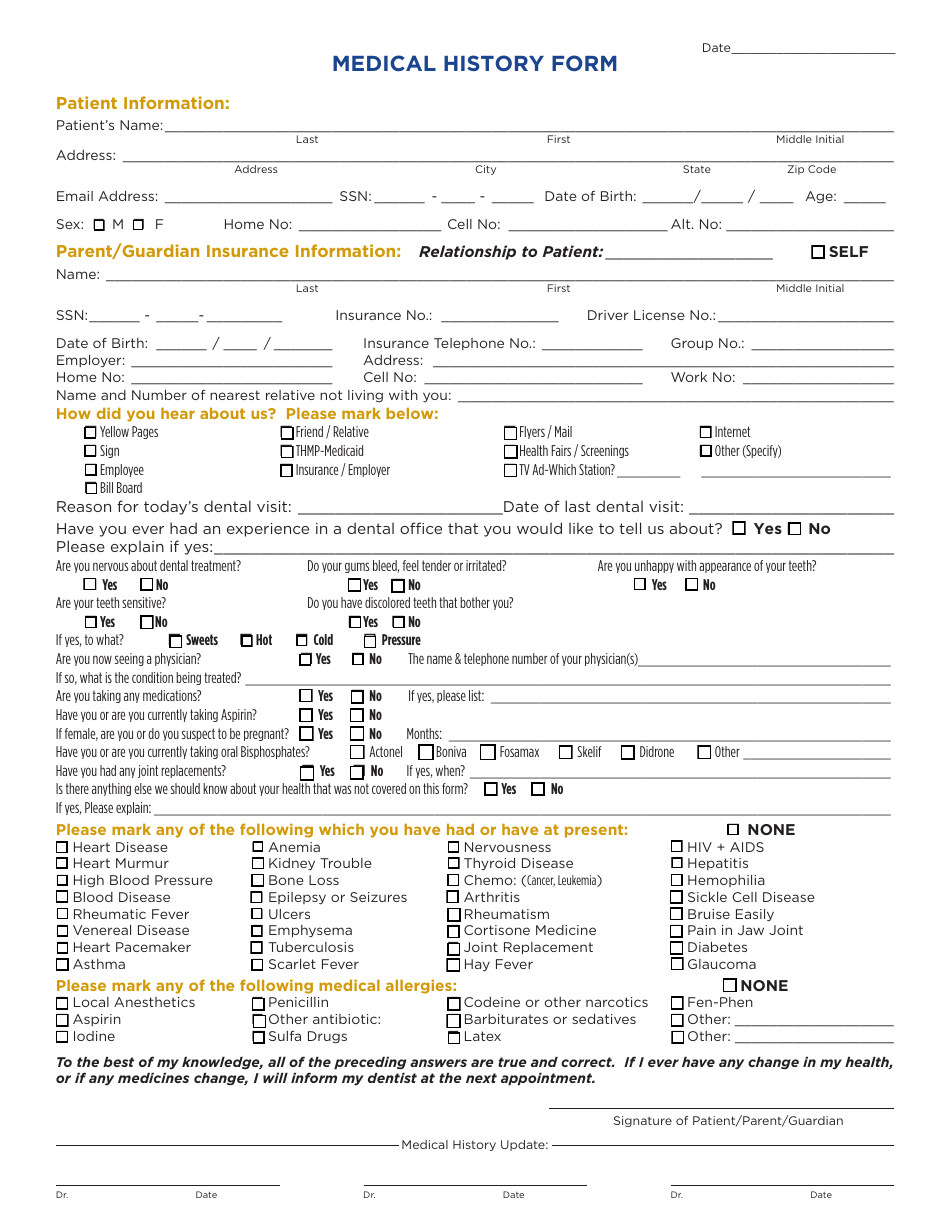
Printable Medical History Form For Dental Office - I understand that providing incorrect information can be. Date of your last dental exam: To the best of my knowledge, the questions on this form have been accurately answered. What was done at that time? Your response to indicate if you have or have not had any of the following diseases or problems. How would you describe your current dental problem? Have you had a serious/difficult problem associated with any previous dental treatment? It is my responsibility to inform the dental office of any changes in medical status. This form is designed to collect patient information, medical history, and authorization related to dental care. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers.
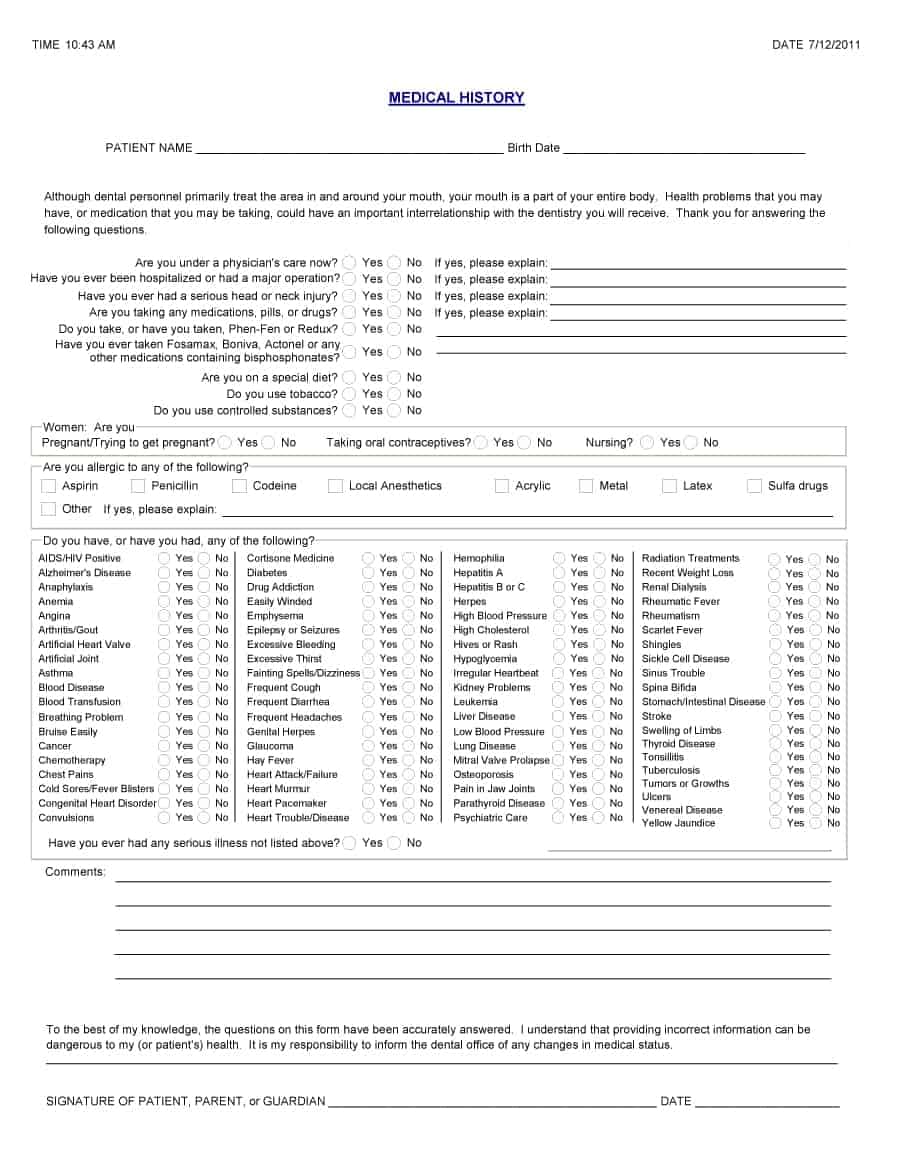
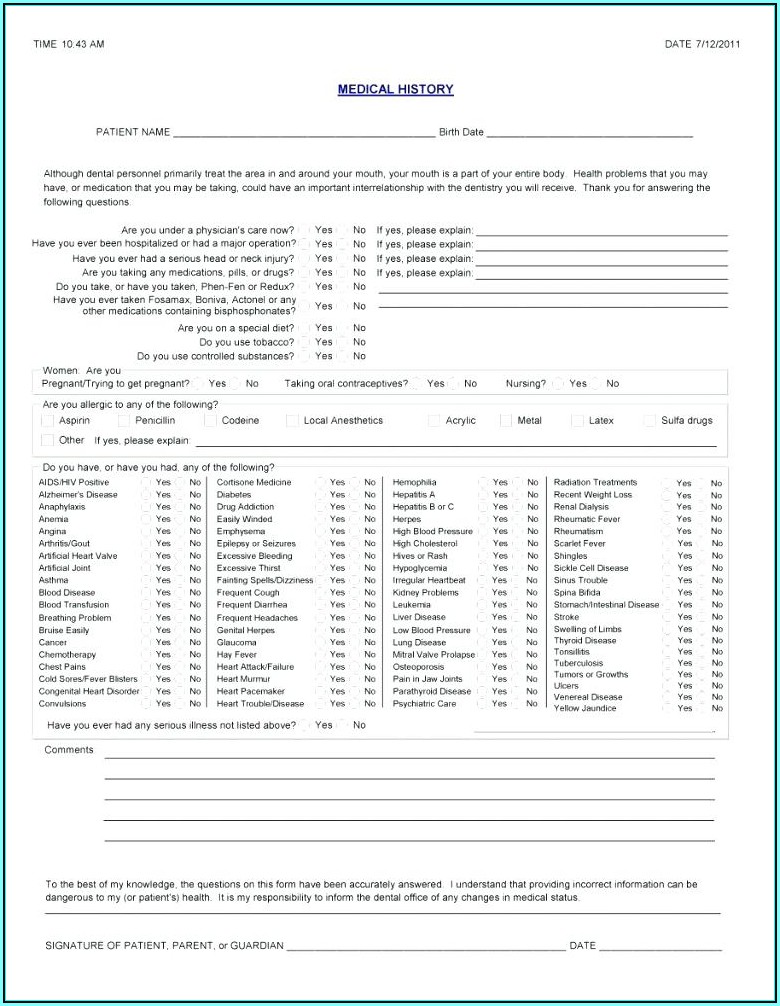
How would you describe your current dental problem? It is my responsibility to inform the dental office of any changes in medical status. What was done at that time? This form is designed to collect patient information, medical history, and authorization related to dental care. It helps dental staff understand your health. Date of your last dental exam: To the best of my knowledge, the questions on this form have been accurately answered. I understand that providing incorrect information can be. Have you had a serious/difficult problem associated with any previous dental treatment? Your response to indicate if you have or have not had any of the following diseases or problems.
To the best of my knowledge, the questions on this form have been accurately answered. It helps dental staff understand your health. How would you describe your current dental problem? It is my responsibility to inform the dental office of any changes in medical status. Date of your last dental exam: Have you had a serious/difficult problem associated with any previous dental treatment? The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. Signature of patient, parent, or guardian _____ date _____. This form is designed to collect patient information, medical history, and authorization related to dental care. I understand that providing incorrect information can be.

Printable Medical History Form For Dental Office Printable Word Searches
It is my responsibility to inform the dental office of any changes in medical status. What was done at that time? It helps dental staff understand your health. Have you had a serious/difficult problem associated with any previous dental treatment? Signature of patient, parent, or guardian _____ date _____.
Printable Medical History Form For Dental Office
Your response to indicate if you have or have not had any of the following diseases or problems. How would you describe your current dental problem? What was done at that time? The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. This form is designed to collect.

the medical history worksheet is shown in this file, and contains
It is my responsibility to inform the dental office of any changes in medical status. To the best of my knowledge, the questions on this form have been accurately answered. This form is designed to collect patient information, medical history, and authorization related to dental care. Signature of patient, parent, or guardian _____ date _____. Have you had a serious/difficult.

Sample Medical History Form Dental Office Classles Democracy
Signature of patient, parent, or guardian _____ date _____. Your response to indicate if you have or have not had any of the following diseases or problems. To the best of my knowledge, the questions on this form have been accurately answered. This form is designed to collect patient information, medical history, and authorization related to dental care. What was.

Printable Medical History Form For Dental Office Printable Forms Free
Signature of patient, parent, or guardian _____ date _____. The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. Date of your last dental exam: It helps dental staff understand your health. What was done at that time?
General Printable Medical History Form Template
It helps dental staff understand your health. How would you describe your current dental problem? It is my responsibility to inform the dental office of any changes in medical status. Date of your last dental exam: To the best of my knowledge, the questions on this form have been accurately answered.
Printable Medical History Form For Dental Office Printable Forms Free
Signature of patient, parent, or guardian _____ date _____. What was done at that time? The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. To the best of my knowledge, the questions on this form have been accurately answered. How would you describe your current dental problem?

Printable Medical History Form For Dental Office Printable Word Searches
Your response to indicate if you have or have not had any of the following diseases or problems. Date of your last dental exam: Signature of patient, parent, or guardian _____ date _____. How would you describe your current dental problem? This form is designed to collect patient information, medical history, and authorization related to dental care.
Free Dental Charting Forms Form Resume Examples AjYdX7qbYl
What was done at that time? Your response to indicate if you have or have not had any of the following diseases or problems. Have you had a serious/difficult problem associated with any previous dental treatment? The american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers. It is.

Printable Medical History Form For Dental Office Printable Word Searches
This form is designed to collect patient information, medical history, and authorization related to dental care. It is my responsibility to inform the dental office of any changes in medical status. Your response to indicate if you have or have not had any of the following diseases or problems. How would you describe your current dental problem? Signature of patient,.
I Understand That Providing Incorrect Information Can Be.
This form is designed to collect patient information, medical history, and authorization related to dental care. To the best of my knowledge, the questions on this form have been accurately answered. What was done at that time? Your response to indicate if you have or have not had any of the following diseases or problems.
The American Dental Association (Ada) Offers A Comprehensive Health History Form, For Adults Or Children In Both English And Spanish, That Covers.
Signature of patient, parent, or guardian _____ date _____. It is my responsibility to inform the dental office of any changes in medical status. Have you had a serious/difficult problem associated with any previous dental treatment? Date of your last dental exam:
How Would You Describe Your Current Dental Problem?
It helps dental staff understand your health.