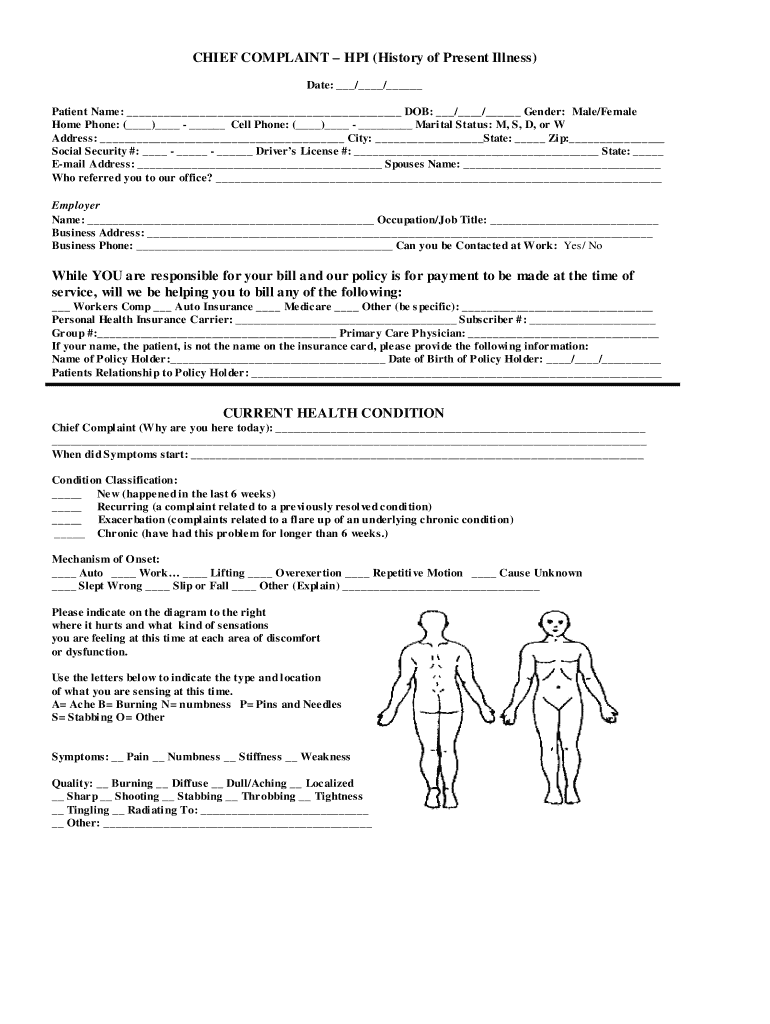
Patient Chief Complaint Form
Patient Chief Complaint Form - Approved by the state to see work comp injuries and the patient will be responsible.) i hereby give consent for. Why are you here today? ______________________________________________________________________________ did your problem result from a specific injury? _____ _____ _____ _____ first mi last preferred name Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o u seizures stroke hepatitis migraines copd/emphysema hiv/aids. By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury.
Why are you here today? By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Approved by the state to see work comp injuries and the patient will be responsible.) i hereby give consent for. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. _____ _____ _____ _____ first mi last preferred name ______________________________________________________________________________ did your problem result from a specific injury? Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o u seizures stroke hepatitis migraines copd/emphysema hiv/aids.
_____ _____ _____ _____ first mi last preferred name By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Why are you here today? ______________________________________________________________________________ did your problem result from a specific injury? Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o u seizures stroke hepatitis migraines copd/emphysema hiv/aids. Approved by the state to see work comp injuries and the patient will be responsible.) i hereby give consent for. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury.
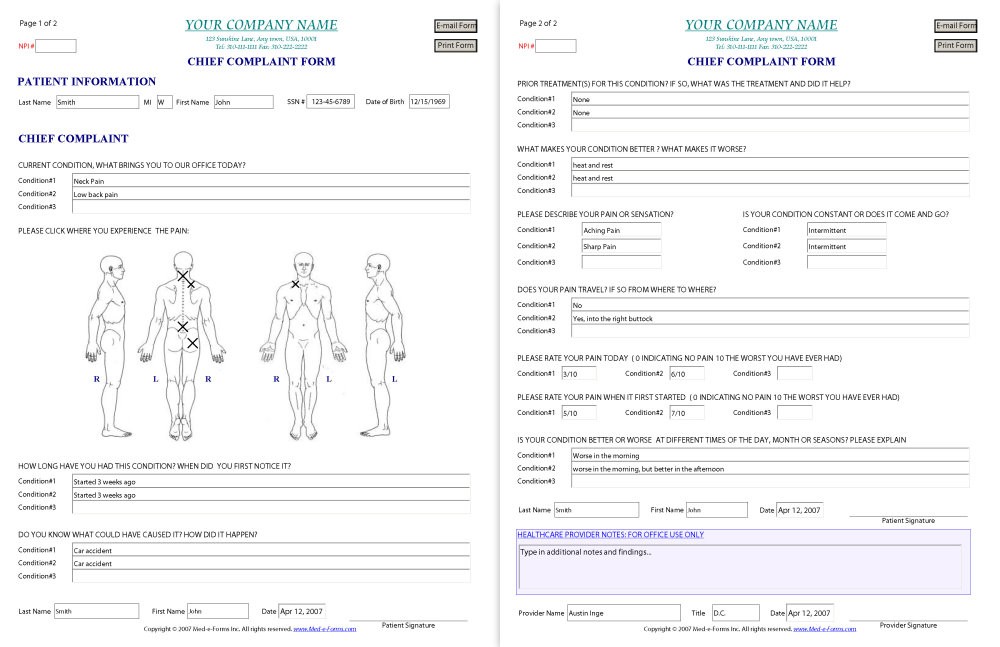
Chief Complaint Form Sample Main Window MedeForms Computer
Why are you here today? _____ _____ _____ _____ first mi last preferred name Approved by the state to see work comp injuries and the patient will be responsible.) i hereby give consent for. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. By signing this form, i permit baptist medical group.
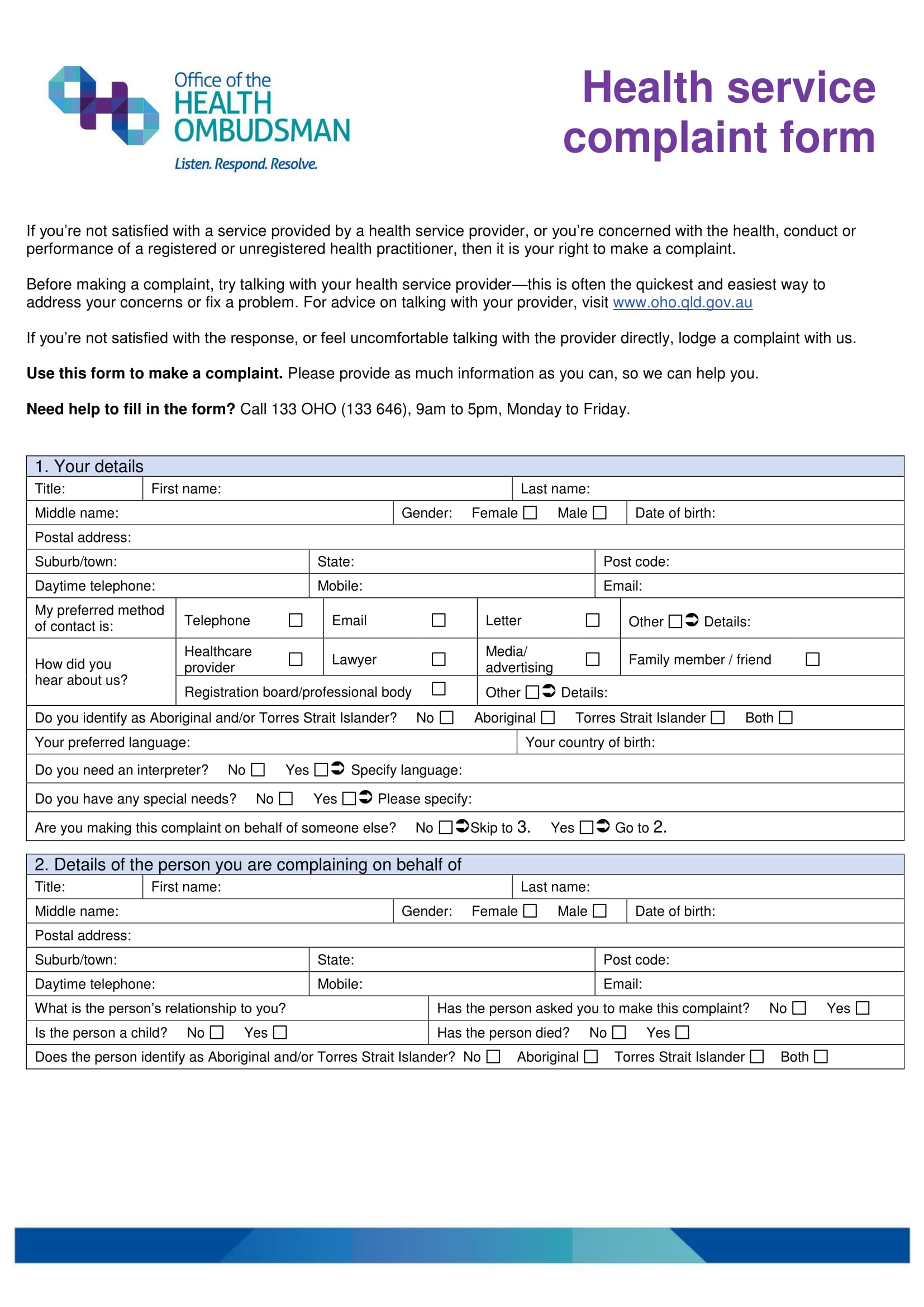
FREE 11+ Health Complaint Form Samples in PDF MS Word
By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. ______________________________________________________________________________ did your problem result from a specific injury? Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o.
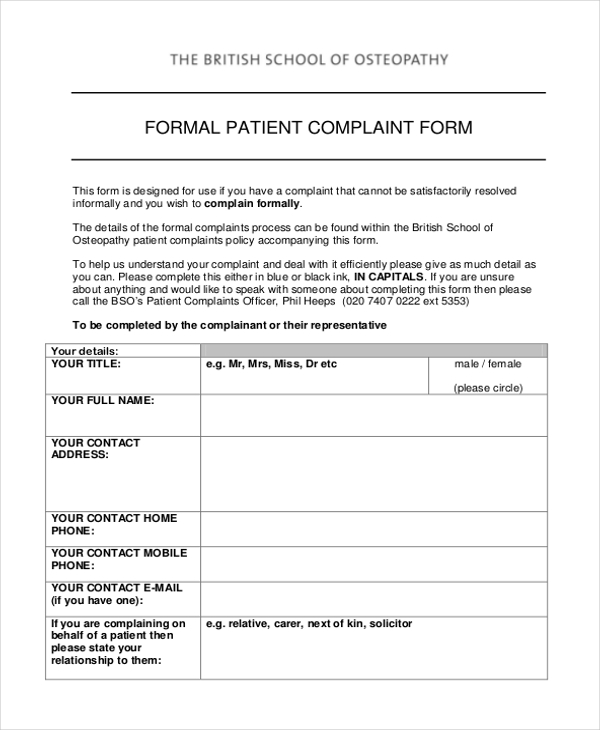
FREE 11+ Sample Patient Complaint Forms in PDF Word
By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Approved by the state to see work comp injuries and the patient will be responsible.) i hereby give consent for. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. Why are.
Soundcare Chiropractic Fill Online, Printable, Fillable, Blank
Approved by the state to see work comp injuries and the patient will be responsible.) i hereby give consent for. By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. Current medical.
FREE 8+ Patient Complaint Forms in PDF MS Word
Why are you here today? Approved by the state to see work comp injuries and the patient will be responsible.) i hereby give consent for. Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o u seizures stroke hepatitis migraines.

Save time and money on Health professions complaint form and BuyerQuest
______________________________________________________________________________ did your problem result from a specific injury? By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below. Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o.

Chief Complaint Format PDF Medicine Human Head And Neck
______________________________________________________________________________ did your problem result from a specific injury? Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o u seizures stroke hepatitis migraines copd/emphysema hiv/aids. _____ _____ _____ _____ first mi last preferred name By signing this form, i.

EMR > Charting > How to fill out Chief Complaint?
Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o u seizures stroke hepatitis migraines copd/emphysema hiv/aids. By signing this form, i permit.
FREE 23+ Sample Complaint Forms in PDF MS Word Excel
Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o u seizures stroke hepatitis migraines copd/emphysema hiv/aids. _____ _____ _____ _____ first mi last preferred name ______________________________________________________________________________ did your problem result from a specific injury? By signing this form, i.
FREE 37+ Complaint Forms in MS Word
Approved by the state to see work comp injuries and the patient will be responsible.) i hereby give consent for. Current medical history p l e a s e c h e c k a l l t h a t a p p l y t o y o u seizures stroke hepatitis migraines copd/emphysema hiv/aids. _____ _____ _____.
Current Medical History P L E A S E C H E C K A L L T H A T A P P L Y T O Y O U Seizures Stroke Hepatitis Migraines Copd/Emphysema Hiv/Aids.
_____ _____ _____ _____ first mi last preferred name Approved by the state to see work comp injuries and the patient will be responsible.) i hereby give consent for. Please complete the following section only if your chief complaint/symptoms were due to an accident or injury. By signing this form, i permit baptist medical group (bmg) staff to discuss information about me with the people listed below.
______________________________________________________________________________ Did Your Problem Result From A Specific Injury?
Why are you here today?