Medical Records Release Form Florida
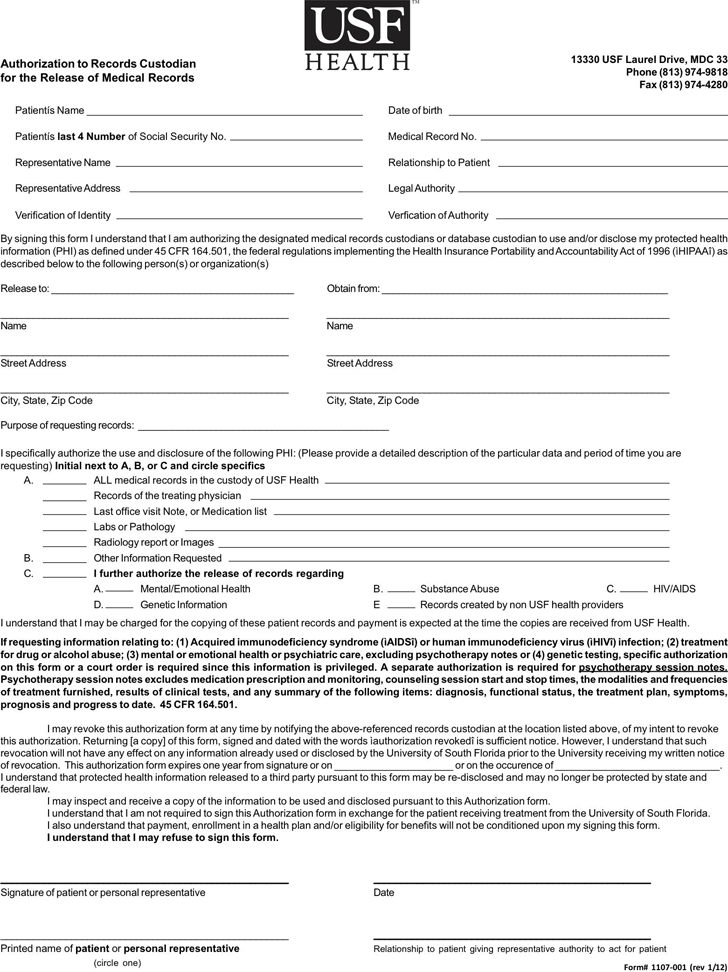
Medical Records Release Form Florida - This form specifically includes authorization to provide documents related to sensitive health conditions including: Fill in the patient’s information and requestor’s name and contact number. Complete all sections of the authorization to disclose confidential information form;. Abstract [*a summary of your visit that contains pertinent information. Release information from (check all that apply): This hipaa release form florida enables patients to permit any person or third parties to have access to private health records. I authorize cleveland clinic florida to use or disclose my health information (including the highly confidential i selected. How to obtain copies of your medical record: Fill in the person, provider, or facility that is. If you are a legal representative of the person whose information you are requesting, you must provide documentation proving your legal.
Fill in the person, provider, or facility that is. I authorize cleveland clinic florida to use or disclose my health information (including the highly confidential i selected. Release information from (check all that apply): Complete all sections of the authorization to disclose confidential information form;. If you are a legal representative of the person whose information you are requesting, you must provide documentation proving your legal. Fill in the patient’s information and requestor’s name and contact number. This form specifically includes authorization to provide documents related to sensitive health conditions including: This hipaa release form florida enables patients to permit any person or third parties to have access to private health records. How to obtain copies of your medical record: Abstract [*a summary of your visit that contains pertinent information.
Complete all sections of the authorization to disclose confidential information form;. How to obtain copies of your medical record: This form specifically includes authorization to provide documents related to sensitive health conditions including: This hipaa release form florida enables patients to permit any person or third parties to have access to private health records. Fill in the patient’s information and requestor’s name and contact number. Fill in the person, provider, or facility that is. Release information from (check all that apply): I authorize cleveland clinic florida to use or disclose my health information (including the highly confidential i selected. If you are a legal representative of the person whose information you are requesting, you must provide documentation proving your legal. Abstract [*a summary of your visit that contains pertinent information.

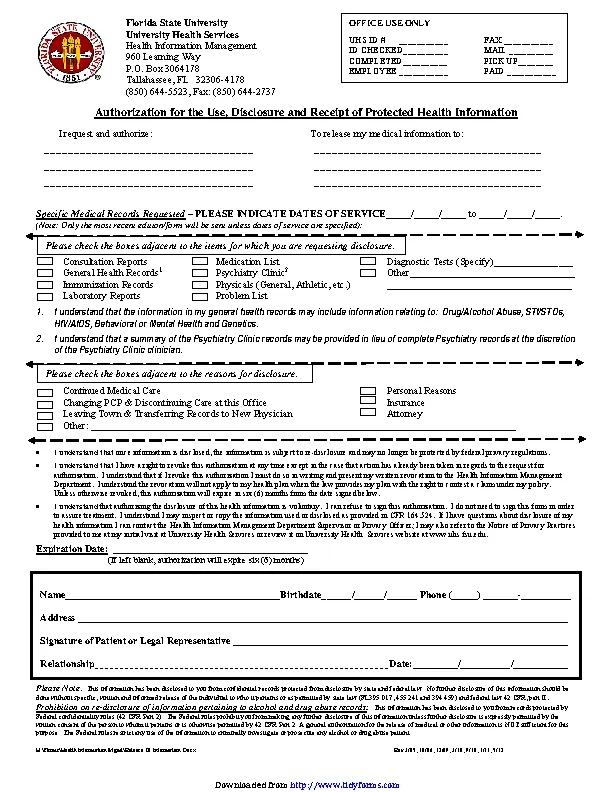
AUTHORIZATION TO RELEASE MEDICAL RECORD INFORMATION Fill and Sign
I authorize cleveland clinic florida to use or disclose my health information (including the highly confidential i selected. Fill in the person, provider, or facility that is. This form specifically includes authorization to provide documents related to sensitive health conditions including: Abstract [*a summary of your visit that contains pertinent information. This hipaa release form florida enables patients to permit.

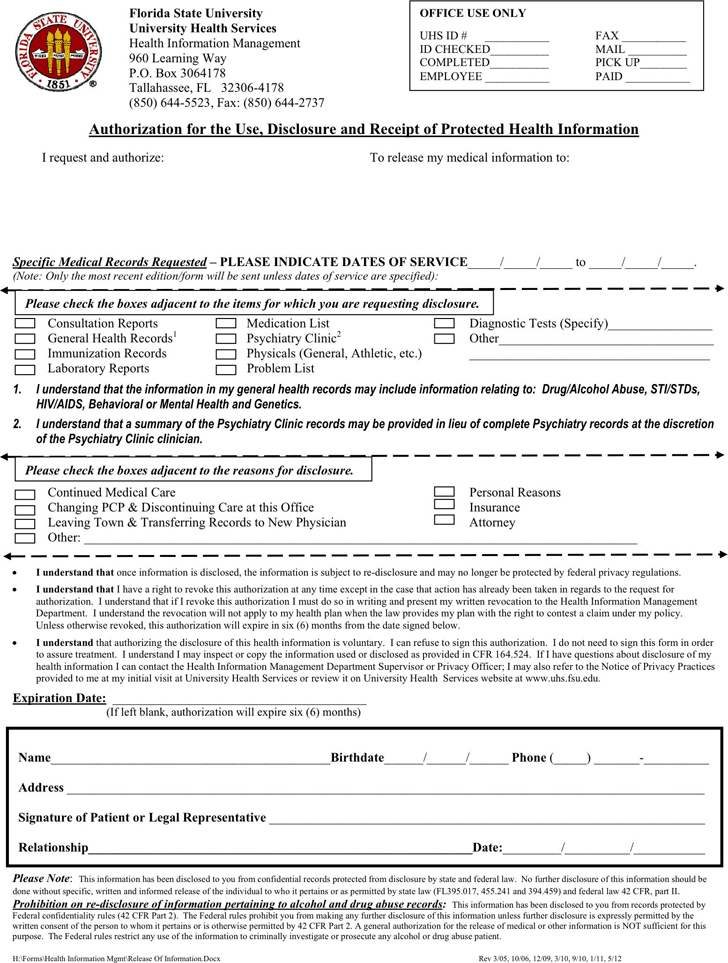
Free Florida Medical Records Release Form PDF 60KB 2 Page(s
Fill in the patient’s information and requestor’s name and contact number. Release information from (check all that apply): If you are a legal representative of the person whose information you are requesting, you must provide documentation proving your legal. Fill in the person, provider, or facility that is. This form specifically includes authorization to provide documents related to sensitive health.
Medical Records Release Template Free Template Download,Customize and
Abstract [*a summary of your visit that contains pertinent information. Complete all sections of the authorization to disclose confidential information form;. Release information from (check all that apply): This hipaa release form florida enables patients to permit any person or third parties to have access to private health records. Fill in the patient’s information and requestor’s name and contact number.
Medical Release Forms Archives Page 39 of 41 PDFSimpli
If you are a legal representative of the person whose information you are requesting, you must provide documentation proving your legal. Fill in the patient’s information and requestor’s name and contact number. I authorize cleveland clinic florida to use or disclose my health information (including the highly confidential i selected. How to obtain copies of your medical record: Complete all.

Medical Release Form Template 30+ Medical Release Form Templates
Complete all sections of the authorization to disclose confidential information form;. Fill in the patient’s information and requestor’s name and contact number. Fill in the person, provider, or facility that is. This hipaa release form florida enables patients to permit any person or third parties to have access to private health records. If you are a legal representative of the.
Free Florida Medical Records Release Form PDF 219KB 1 Page(s)
Complete all sections of the authorization to disclose confidential information form;. Abstract [*a summary of your visit that contains pertinent information. If you are a legal representative of the person whose information you are requesting, you must provide documentation proving your legal. Fill in the patient’s information and requestor’s name and contact number. I authorize cleveland clinic florida to use.
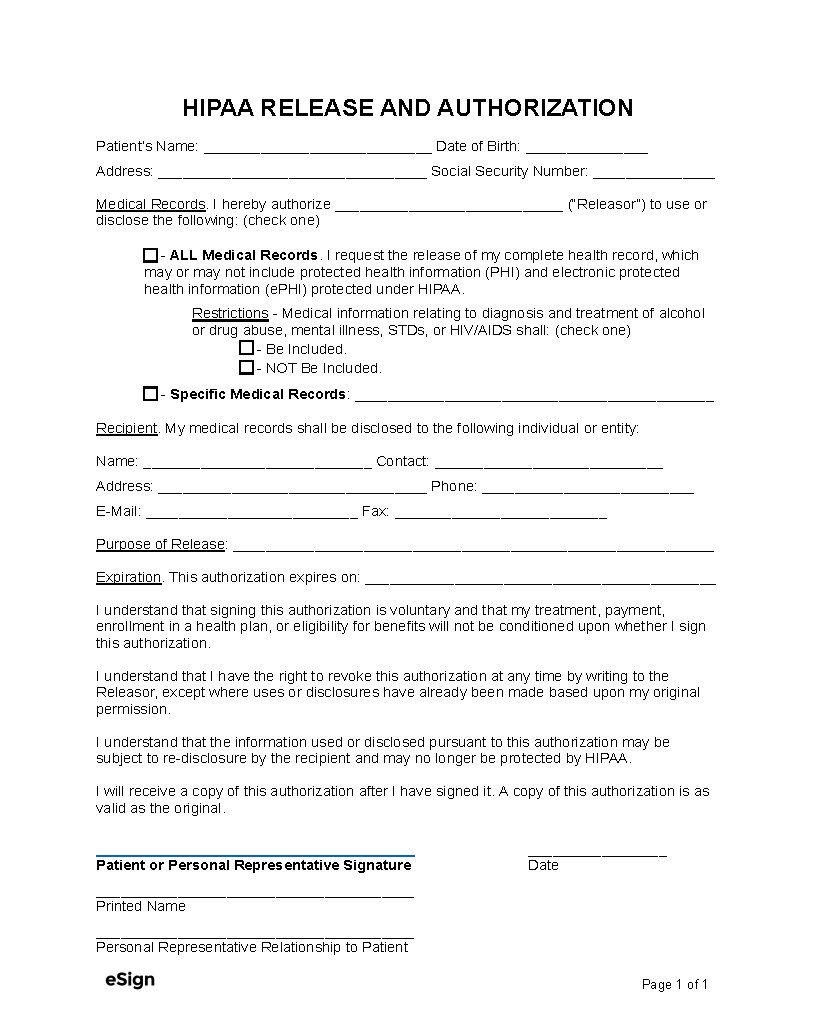
Free Medical Records Release Form (HIPAA) PDF Word
This form specifically includes authorization to provide documents related to sensitive health conditions including: Fill in the patient’s information and requestor’s name and contact number. Abstract [*a summary of your visit that contains pertinent information. Fill in the person, provider, or facility that is. I authorize cleveland clinic florida to use or disclose my health information (including the highly confidential.
Printable Patient Medical Record Template
Fill in the person, provider, or facility that is. How to obtain copies of your medical record: Complete all sections of the authorization to disclose confidential information form;. Abstract [*a summary of your visit that contains pertinent information. Release information from (check all that apply):

Florida Medical Records Release Form Download Free Printable Blank
This hipaa release form florida enables patients to permit any person or third parties to have access to private health records. If you are a legal representative of the person whose information you are requesting, you must provide documentation proving your legal. Abstract [*a summary of your visit that contains pertinent information. Fill in the person, provider, or facility that.
Medical Release Forms Printable
Fill in the patient’s information and requestor’s name and contact number. This form specifically includes authorization to provide documents related to sensitive health conditions including: Complete all sections of the authorization to disclose confidential information form;. How to obtain copies of your medical record: Abstract [*a summary of your visit that contains pertinent information.
If You Are A Legal Representative Of The Person Whose Information You Are Requesting, You Must Provide Documentation Proving Your Legal.
How to obtain copies of your medical record: This form specifically includes authorization to provide documents related to sensitive health conditions including: Release information from (check all that apply): I authorize cleveland clinic florida to use or disclose my health information (including the highly confidential i selected.
Complete All Sections Of The Authorization To Disclose Confidential Information Form;.
Abstract [*a summary of your visit that contains pertinent information. This hipaa release form florida enables patients to permit any person or third parties to have access to private health records. Fill in the patient’s information and requestor’s name and contact number. Fill in the person, provider, or facility that is.