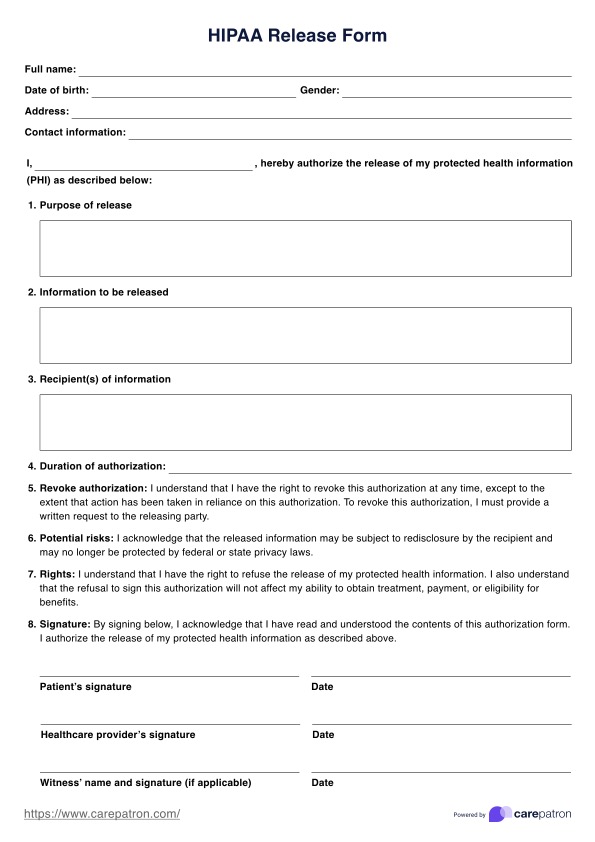
Hipaa Release Form Ohio
Hipaa Release Form Ohio - + i understand that this authorization may. + i understand that my records/protected health information cannot be released unless i sign this form. The purpose of this release is to ensure prompt payment of my insurance premiums. Cdjfs authorization template (pdf format / ms word). As such, any communication from representatives of the. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric. List of hipaa reference links such as privacy information, forms, and disclosures. Elease of information from covered entities. Standard authorization form contains two separate forms. Form a is an authorization for.
Elease of information from covered entities. Cdjfs authorization template (pdf format / ms word). Standard authorization form contains two separate forms. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric. As such, any communication from representatives of the. Form a is an authorization for. The purpose of this release is to ensure prompt payment of my insurance premiums. + i understand that this authorization may. List of hipaa reference links such as privacy information, forms, and disclosures. + i understand that my records/protected health information cannot be released unless i sign this form.
As such, any communication from representatives of the. Cdjfs authorization template (pdf format / ms word). The health insurance portability and accountability act (hipaa) of 1996 is a federal law impacting both consumers and providers of. Form a is an authorization for. Standard authorization form contains two separate forms. The purpose of this release is to ensure prompt payment of my insurance premiums. Elease of information from covered entities. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric. + i understand that my records/protected health information cannot be released unless i sign this form. + i understand that this authorization may.
Form 104 Ohio Northern University Hipaa Compliant Authorization For
Cdjfs authorization template (pdf format / ms word). The purpose of this release is to ensure prompt payment of my insurance premiums. + i understand that my records/protected health information cannot be released unless i sign this form. + i understand that this authorization may. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of.
Hipaa Printable Forms
+ i understand that my records/protected health information cannot be released unless i sign this form. Cdjfs authorization template (pdf format / ms word). List of hipaa reference links such as privacy information, forms, and disclosures. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric. Standard authorization form contains two separate forms.

Hipaa Letter Medical Collection Template
Form a is an authorization for. The health insurance portability and accountability act (hipaa) of 1996 is a federal law impacting both consumers and providers of. + i understand that my records/protected health information cannot be released unless i sign this form. The purpose of this release is to ensure prompt payment of my insurance premiums. Elease of information from.
HIPAA Release Form Illinois & Example Free PDF Download
Standard authorization form contains two separate forms. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric. Form a is an authorization for. + i understand that my records/protected health information cannot be released unless i sign this form. As such, any communication from representatives of the.
Medical Release Forms Archives Page 3 of 41 PDFSimpli
Cdjfs authorization template (pdf format / ms word). + i understand that my records/protected health information cannot be released unless i sign this form. Standard authorization form contains two separate forms. List of hipaa reference links such as privacy information, forms, and disclosures. As such, any communication from representatives of the.
Printable Hipaa Release Form
Form a is an authorization for. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric. As such, any communication from representatives of the. + i understand that my records/protected health information cannot be released unless i sign this form. + i understand that this authorization may.
HIPAA Medical Release Form & Example Free PDF Download
Form a is an authorization for. As such, any communication from representatives of the. The health insurance portability and accountability act (hipaa) of 1996 is a federal law impacting both consumers and providers of. Standard authorization form contains two separate forms. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric.

Hipaa Free Printable Form For Ohio Form Printable Forms Free Online
As such, any communication from representatives of the. + i understand that my records/protected health information cannot be released unless i sign this form. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric. + i understand that this authorization may. Standard authorization form contains two separate forms.
Hipaa Forms Florida Printable
+ i understand that this authorization may. + i understand that my records/protected health information cannot be released unless i sign this form. The health insurance portability and accountability act (hipaa) of 1996 is a federal law impacting both consumers and providers of. Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric..

Hipaa Fillable Fill Online, Printable, Fillable, Blank pdfFiller
Records released pursuant to this authorization may include information concerning testing, diagnosis or treatment of hiv/aids, psychiatric. Elease of information from covered entities. The purpose of this release is to ensure prompt payment of my insurance premiums. The health insurance portability and accountability act (hipaa) of 1996 is a federal law impacting both consumers and providers of. Form a is.
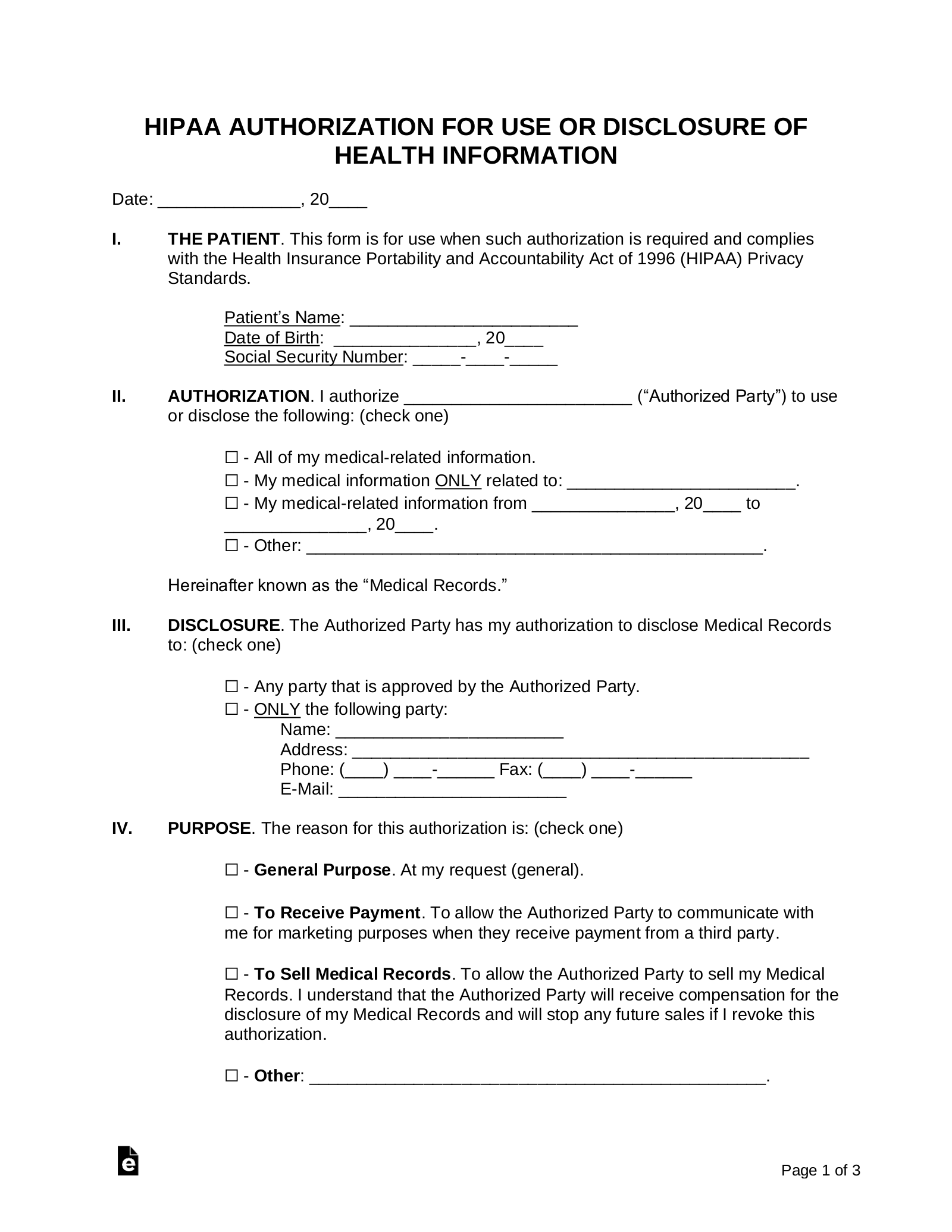
Standard Authorization Form Contains Two Separate Forms.
The health insurance portability and accountability act (hipaa) of 1996 is a federal law impacting both consumers and providers of. Elease of information from covered entities. Form a is an authorization for. + i understand that this authorization may.
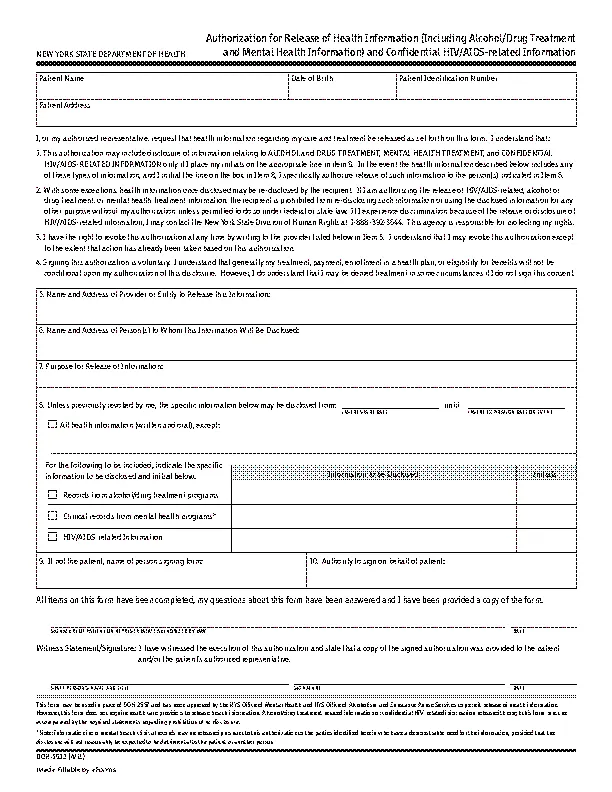
Records Released Pursuant To This Authorization May Include Information Concerning Testing, Diagnosis Or Treatment Of Hiv/Aids, Psychiatric.
As such, any communication from representatives of the. The purpose of this release is to ensure prompt payment of my insurance premiums. List of hipaa reference links such as privacy information, forms, and disclosures. Cdjfs authorization template (pdf format / ms word).