Healthfirst Appeal Form
Healthfirst Appeal Form - File an appeal if your request is denied. Use one form for each disputed claim. Provide a clear rationale and any additional documentation (such as medical records) to support your. A copy of the provider claim dispute request. Use this form to name someone to act. Designate a representative to assist with authorizations, complaints, grievances, and appeals. Providers may submit disputes by sending the dispute via fax, mail or through the provider portal. An appeal is a formal way of askingus to review and change a coverage decision we made. If your request for coverage of medical care is denied, you or your authorized. If my request is denied, how can i appeal?
Use one form for each disputed claim. Providers may submit disputes by sending the dispute via fax, mail or through the provider portal. A copy of the provider claim dispute request. If your request for coverage of medical care is denied, you or your authorized. Use this form to name someone to act. File an appeal if your request is denied. If my request is denied, how can i appeal? An appeal is a formal way of askingus to review and change a coverage decision we made. Provide a clear rationale and any additional documentation (such as medical records) to support your. Designate a representative to assist with authorizations, complaints, grievances, and appeals.
Use one form for each disputed claim. An appeal is a formal way of askingus to review and change a coverage decision we made. Provide a clear rationale and any additional documentation (such as medical records) to support your. If my request is denied, how can i appeal? Providers may submit disputes by sending the dispute via fax, mail or through the provider portal. Designate a representative to assist with authorizations, complaints, grievances, and appeals. File an appeal if your request is denied. If your request for coverage of medical care is denied, you or your authorized. Use this form to name someone to act. A copy of the provider claim dispute request.
Healthfirst Renewal 20122024 Form Fill Out and Sign Printable PDF
A copy of the provider claim dispute request. If my request is denied, how can i appeal? File an appeal if your request is denied. Providers may submit disputes by sending the dispute via fax, mail or through the provider portal. Designate a representative to assist with authorizations, complaints, grievances, and appeals.
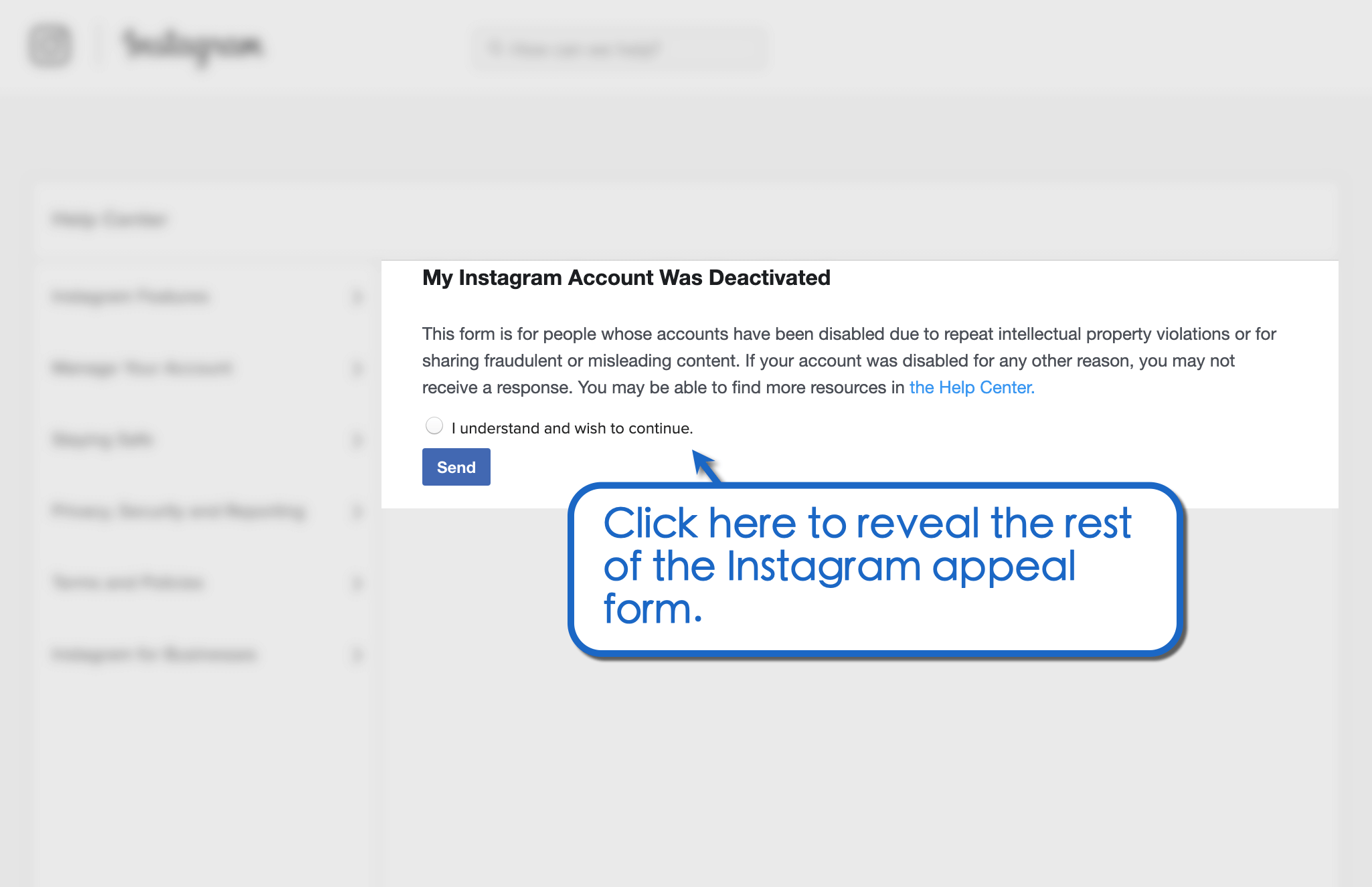
How to Use the Instagram Appeal Form for Banned Profiles Vista Social
File an appeal if your request is denied. If my request is denied, how can i appeal? If your request for coverage of medical care is denied, you or your authorized. Use one form for each disputed claim. Use this form to name someone to act.
20212023 ZA NSFAS Appeal Form Fill Online, Printable, Fillable, Blank
File an appeal if your request is denied. An appeal is a formal way of askingus to review and change a coverage decision we made. Use this form to name someone to act. Providers may submit disputes by sending the dispute via fax, mail or through the provider portal. If your request for coverage of medical care is denied, you.

1st Appeal Format RTI 19 1 2005 PDF
Use this form to name someone to act. Providers may submit disputes by sending the dispute via fax, mail or through the provider portal. If my request is denied, how can i appeal? A copy of the provider claim dispute request. Provide a clear rationale and any additional documentation (such as medical records) to support your.
20142024 Form CA EDD DE 1000M/C Fill Online, Printable, Fillable
Provide a clear rationale and any additional documentation (such as medical records) to support your. Designate a representative to assist with authorizations, complaints, grievances, and appeals. If my request is denied, how can i appeal? If your request for coverage of medical care is denied, you or your authorized. A copy of the provider claim dispute request.
9+ Sample Caremark Prior Authorization Forms Sample Templates
An appeal is a formal way of askingus to review and change a coverage decision we made. File an appeal if your request is denied. Use one form for each disputed claim. Provide a clear rationale and any additional documentation (such as medical records) to support your. If my request is denied, how can i appeal?

Hudson Health Plan Medication Prior Authorization Form
File an appeal if your request is denied. Providers may submit disputes by sending the dispute via fax, mail or through the provider portal. Designate a representative to assist with authorizations, complaints, grievances, and appeals. If your request for coverage of medical care is denied, you or your authorized. Provide a clear rationale and any additional documentation (such as medical.
22 Medicare Prior Authorization Form Templates free to download in PDF
An appeal is a formal way of askingus to review and change a coverage decision we made. Designate a representative to assist with authorizations, complaints, grievances, and appeals. A copy of the provider claim dispute request. Use one form for each disputed claim. Use this form to name someone to act.
Coverage Determination, Appeals and Payment Request Fill Out and Sign
A copy of the provider claim dispute request. File an appeal if your request is denied. An appeal is a formal way of askingus to review and change a coverage decision we made. Provide a clear rationale and any additional documentation (such as medical records) to support your. Use this form to name someone to act.

Fillable Online HealthFirst NY POD Req Form 2021 (49648 Activated
If my request is denied, how can i appeal? File an appeal if your request is denied. Use one form for each disputed claim. Designate a representative to assist with authorizations, complaints, grievances, and appeals. Provide a clear rationale and any additional documentation (such as medical records) to support your.
Designate A Representative To Assist With Authorizations, Complaints, Grievances, And Appeals.
If my request is denied, how can i appeal? If your request for coverage of medical care is denied, you or your authorized. Use this form to name someone to act. A copy of the provider claim dispute request.
File An Appeal If Your Request Is Denied.
Provide a clear rationale and any additional documentation (such as medical records) to support your. Providers may submit disputes by sending the dispute via fax, mail or through the provider portal. An appeal is a formal way of askingus to review and change a coverage decision we made. Use one form for each disputed claim.